David Wallace-Wells with the best piece I’ve read on Covid in quite a while (this one gets the gift link):
Nationally, the BA.5 wave does not appear to have crested yet, but so far deaths, while rising, are doing so relatively slowly. Pull far enough back in looking at the graphs and it’s hard to even see the increase. Hospitalizations have doubled roughly since May but are still only a quarter as high as they were at the peak of the initial Omicron wave and well below any of the pandemic’s previous peaks. I.C.U. admissions have barely budged.
How can you characterize this dynamic, or make sense of it? Wave after wave of infection passing through, but almost in the background; hospitalizations and deaths bumping up and down, but mostly within a relatively narrow range, and much lower, relative to caseloads, than we remember even from the first Omicron wave, let alone Delta before that and the waves of 2020 still earlier.
One word for it is “endemic,” says Trevor Bedford, a computational virologist at the Fred Hutchinson Cancer Center in Seattle and among the most careful and dependable soothsayers of the past two years.
Bedford is reluctant to dwell on semantic debates about what constitutes a “pandemic phase” rather than an “endemic phase” for Covid-19, for instance. But if we insist that the country is still in a pandemic phase, he says, we’re not going to be able to downshift from that anytime soon, since conditions aren’t likely to look very different for years — and the country’s accumulating immunological protection, if imperfect, is still a categorical break from those earlier phases in which we first calibrated our fears. “If we’re saying that we’re still in a pandemic right now, it’s still going to be a pandemic in year seven — we’ll still be in a pandemic then,” Bedford says. “So I think it’s better to acknowledge that we’re at 98 percent of the population having immunity of some form — certainly over 95 percent. There’s not much more that could change in that regard.”
There are technical reasons other epidemiologists would dispute the term “endemic.” With respiratory diseases, it can refer to diseases where the average sick person infects fewer than one new person, and each of this year’s variants is more infectious than that. And while many use “endemic” to imply viral stability, there remains the possibility of a “surprise” in viral evolution, of course; no one I spoke to for this article was comfortable ruling it out…
But in a vernacular sense, the term fits: A large majority of the country has gotten infected with the coronavirus, probably most of us with a strain of Omicron, and 67 percent of us are vaccinated as well (though only 32 percent boosted). And for all the variant-after-variant turbulence of the past few months, from another perspective, the Covid experience in America has been for months in something like a steady state…
This year has been considerably worse than that, largely because it includes the initial arrival of Omicron — which, though often described as “mild,” killed more than 100,000 Americans in the first six weeks of the year. And so although the country’s current trajectory is following an annualized pace of 100,000 deaths, more than 200,000 Americans have died already this year, which implies over 250,000 deaths by the end of 2022.
Michael Mina, an epidemiologist who left Harvard to become the chief scientist at the online medical portal eMed in 2021 after spending most of the pandemic as the country’s leading rapid-testing evangelist, believes it could get worse. With a combination of seasonality and waning immunity among older people, he said, there’s potential for a fall wave of perhaps 1,000 a day. That would bring the number of American deaths, this year, to potentially 300,000 or more…
That toll, 10 times that of recent flu seasons, is smaller, to be sure, than those of the first two years of the pandemic, when just over 400,000 Americans died during both President Donald Trump’s last year in office and in President Biden’s first. But it isn’t that much smaller. Nationally, the infection fatality rate is a fraction of what it once was, but the disease is spreading much more prolifically now and has been all year, which means all told the disease is still generating a quite devastating death toll — particularly among the elderly, who have been accumulating immunity more slowly than the rest of the population and shedding it more quickly.
The way I see it endemic probably is the best description because we do 1) seem to be at a new normal, and 2) this isn’t going away anytime soon. The basic fact seems to me that, within somewhat of a range, we are at a new normal that is simply worse than our old normal. But this is where we are for a while yet until we get those better vaccines we just don’t have enough urgency for. Status quo ante is just not an option. So, yeah, with some modest ups and downs, this is basically just life now.
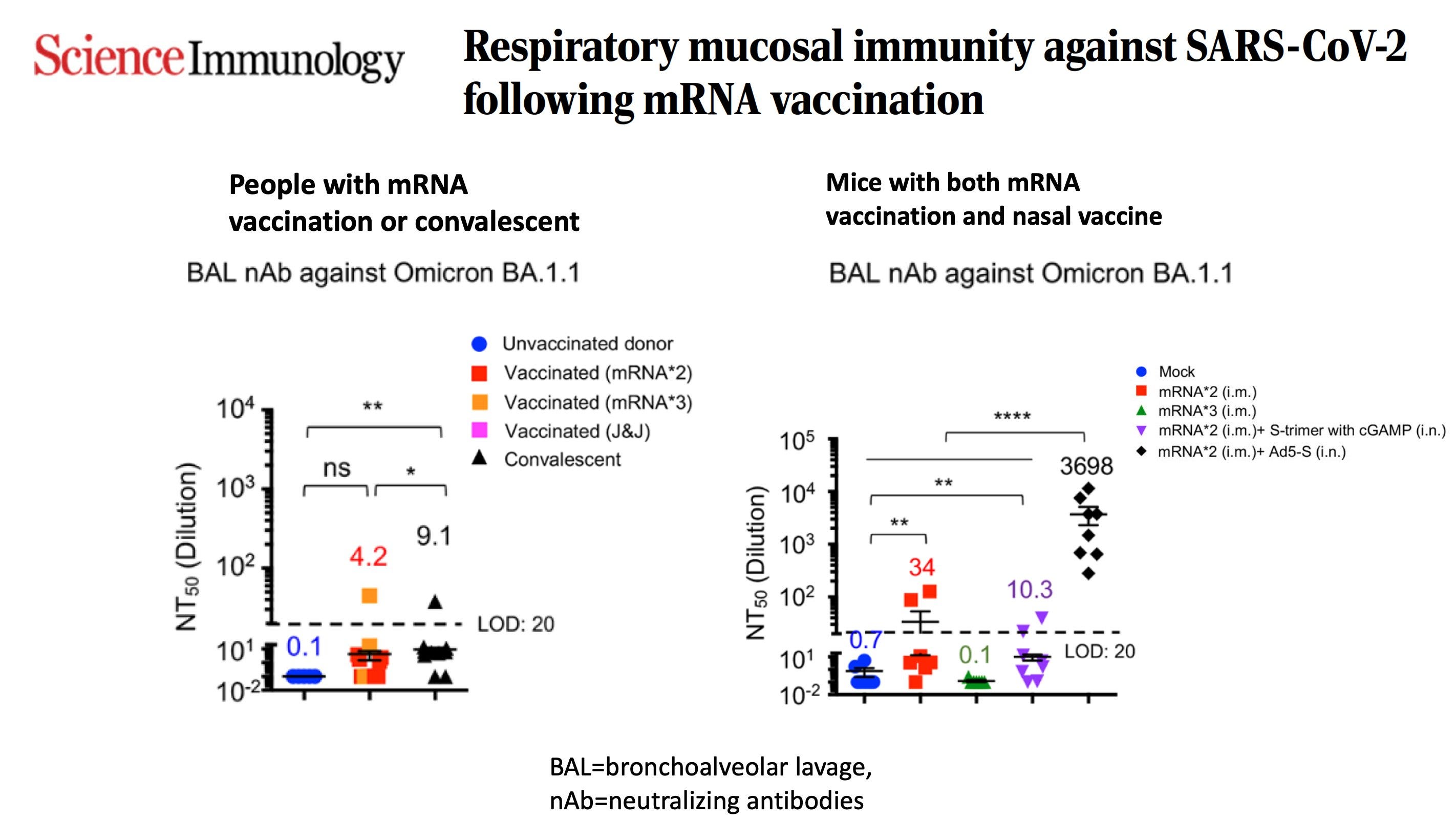
But let me emphasize: the culprit in all of this isn’t our vaccines, which are now providing little to no protection against infections and transmission. They are damn leaky, which only arose from the emergence of Omicron and has gotten progressively worse as we moved to BA.5 . It’s the virus. That’s why we’ve started to see a crack in protection vs. severe disease from vaccines with boosters, as I previously reviewed (boiling frog metaphor). It’s that we have not gotten ahead of the immune escape properties of virus with a bolstered mucosal immunity strategy—local IgA, neutralizing antibodies in the upper airway—via nasal or oral vaccines to solidify our 2nd layer of defense. Or inhaled interferons to jack up our first line of defense. Or developing a variant-proof vaccine…
As Akiko Iwasaki and I wrote last week, it is imperative that we launch a new, major initiative, as we called it Operation Nasal Vaccine, to get ahead of the virus and promote respiratory mucosal immunity.
To summarize a few key points:
There is little to no respiratory mucosal immunity from mRNA vaccines in people vs Omicron
There are 12 nasal vaccines in clinical trials and 4 are late-stage, Phase 3 but there is no government plan for manufacturing, distribution or regulatory review as there was for the original vaccines.
While only 1 nasal spray vaccine is currently available (FluMist for influenza) we have already had marked success on a comparative basis against SAR-CoV-2 for vaccine efficacy and an oral antiviral pill (Paxlovid vs Tamiflu). Furthermore, the biology of the SARS-CoV-2 virus makes it a more favorable target than influenza
Next week the White House is having a next-generation summit meeting to ponder plans for a nasal and universal, variant-proof vaccines. We’ve had enough of pondering……we need action. Let’s hope we finally get the vital support we need to build on our early and momentous success against the virus. It’s still evolving and we are getting further and further behind. We can do this.
I do think, hopefully, we’ll have a new normal that looks like the old normal. But not until we really put the effort into these new vaccines. But, for now, our new normal is a lot better than it was not all that long ago, but alas, it’s going to be a while before we are back to early 2020.
Our dogs have had an effective nasal vaccine for kennel cough for years. There are other nasal meds for canines that are administered through the nose. One is for calming the dog. Maybe we need to start pressuring our elected officials to move on to a nasal vaccine for Covid instead of accepting the status quo.
I’m sure that pharma didn’t know that nasal vaccines would be more effective than IM vaccines at reducing transmission of a virus that infects the nasopharynx.
Fyi, we got some sort of ILI this July 2022 and cleared fever and aches in two days (nausea and diarrhea as well). Mild dizziness, mild fatigue, and mild disorientation lingered for about five days and was likely due to dehydration and hypoglycemia following infection. Anosmia lingered for a few weeks. We suspect it was covid due to the fact that it was going through our metro at the time and due to the anosmia, which is common with covid but not with flu.
Based on some RCTs, we used elderberry concentrate, zinc, and calcifediol to treat.

Our dogs have had an effective nasal vaccine for kennel cough for years. There are other nasal meds for canines that are administered through the nose. One is for calming the dog. Maybe we need to start pressuring our elected officials to move on to a nasal vaccine for Covid instead of accepting the status quo.
I’m sure that pharma didn’t know that nasal vaccines would be more effective than IM vaccines at reducing transmission of a virus that infects the nasopharynx.
Fyi, we got some sort of ILI this July 2022 and cleared fever and aches in two days (nausea and diarrhea as well). Mild dizziness, mild fatigue, and mild disorientation lingered for about five days and was likely due to dehydration and hypoglycemia following infection. Anosmia lingered for a few weeks. We suspect it was covid due to the fact that it was going through our metro at the time and due to the anosmia, which is common with covid but not with flu.
Based on some RCTs, we used elderberry concentrate, zinc, and calcifediol to treat.